In a study of patients with episodic and chronic migraine who experienced 2-4 prior preventive category failures,1
Emgality delivered significant reductions in MHDs1
CONQUER: -4.1 days on Emgality 120 mg (n=232) vs -1.0 day on placebo (n=230) over Months 1 to 3 (baseline: 13.4 vs 13.0) (p<0.0001)1a
aLS means are present.
SELECT IMPORTANT SAFETY INFORMATION
Raynaud's Phenomenon
Development of Raynaud's phenomenon and recurrence or worsening of pre-existing Raynaud's phenomenon have been reported in the postmarketing setting following the use of CGRP antagonists, including Emgality. In reported cases with monoclonal antibody CGRP antagonists, symptom onset occurred after a median of 71 days following dosing. Many of the cases reported serious outcomes, including hospitalizations and disability, generally related to debilitating pain. In most reported cases, discontinuation of the CGRP antagonist resulted in resolution of symptoms.
Emgality should be discontinued if signs or symptoms of Raynaud's phenomenon develop, and patients should be evaluated by a healthcare provider if symptoms do not resolve. Patients with a history of Raynaud's phenomenon should be monitored for, and informed about the possibility of, worsening or recurrence of signs and symptoms.
EMGALITY SIGNIFICANTLY REDUCED THE BURDEN OF MIGRAINE IN BETWEEN ATTACKS2
Patients taking Emgality reported improvement in the burden of migraine in between attacks, as assessed by the MIBS-4.2
Mean change from baseline on the MIBS-4 was greater for patients treated with Emgality vs placebo.
Mean Reduction From Baseline in MIBS-4 at Month 32a
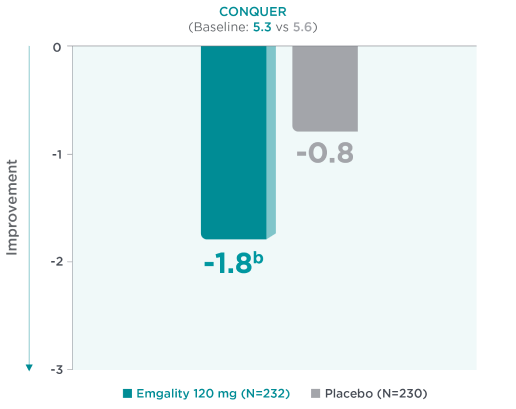
aLS means are presented.2
bNominal p-value ≤0.001 vs placebo.2
Mean reduction from baseline in MIBS-4 scores at Month 3a in CONQUER for Emgality 120 mg (N=232) was -1.8b vs -0.8 with placebo (N=230) (baseline: 5.3 for Emgality vs 5.6 for placebo, respectively).2
Statistical significance does not imply clinically meaningful difference.
Change in MIBS-4 from baseline to Month 3 was evaluated using an ANCOVA model controlling for prespecified effects. For missing MIBS-4 score at Month 3 (9 in placebo, 8 in Emgality 120 mg) LOCF was used. There was no adjustment for multiplicity in the treatment comparisons using the MIBS-4.2
MIBS-4 measures the burden of migraine between attacks, including disruption at work and school, diminished family and social life, difficulty planning, and emotional difficulty.3-5
- MIBS-4 is scored on a scale from 0 to 12. A score of 0 indicates no burden, 1-2 indicates mild burden, 3-4 indicates moderate burden, and scores ≥5 indicate severe burden
ANCOVA=analysis of covariance; LOCF=last observation carried forward; MHD=migraine headache day; MIBS-4=Migraine Interictal Burden Scale-4.
SELECT IMPORTANT SAFETY INFORMATION
Adverse Reactions
The most common adverse reactions (incidence ≥2% and at least 2% greater than placebo) in Emgality clinical studies were injection site reactions.
References
- Mulleners WM, Kim BK, Láinez MJA, et al. Safety and efficacy of galcanezumab in patients for whom previous migraine preventive medication from two to four categories had failed (CONQUER): a multicentre, randomised, double-blind, placebo-controlled, phase 3b trial. Lancet Neurol. 2020;19(10):814-825.
- García-Azorin D, Ford J, Buse DC, et al. Changes in work productivity and interictal burden: results from randomized, double-blind study evaluating galcanezumab in adults with treatment resistant migraine (CONQUER). Presented at: 17th Asian Oceanian Congress of Neurology (AOCN 2021); Taipei, Taiwan; April 1-4, 2021.
- Buse DC, Rupnow MF, Lipton RB. Assessing and managing all aspects of migraine: migraine attacks, migraine-related functional impairment, common comorbidities, and quality of life. Mayo Clin Proc. 2009;84(5):422-435.
- Buse DC, Bigal M, Rupnow M, et al. Development and validation of the Migraine Interictal Burden Scale (MIBS): a self-administered instrument for measuring the burden of migraine between attacks [abstract S05.003]. Neurology. 2007;68(suppl 1):A89.
- Buse DC, Bigal M, Rupnow M, et al. The migraine interictal burden scale (MIBS): results of a population-based validation study. Headache. 2007;47(5):778.